The UNSWOC is committed to train their Trip Leaders in Remote Area First Aid (RAFA), an essential skill to have when leading trips in the outdoors. The following report includes useful advice on what to do regarding common outdoors injuries. For full training, please consider doing a RAFA course.
28-29th July 2018
AllAid First Aid (https://www.allaid.com.au/) at Camp Somerset
For a very valuable report on the First Aid course, including reflections on some learnings, skills, and scenarios, please see Maria's following report:
Participants: Lucy Morrison, Maria Lastra Cagigas, Mira Jordan, Isabella Lowe, Stefanie Tenberg, Ben Wilkinson, Hayden Lobry, Tadeh Karapetian, Abi Prakash, Vicky Chen, Henry Burt, Mackenzie Labine-Romain, Eamonn Colley, Ashley Brennan, David Temesvary, Sid Tinney, Manon Nyssen, Nicola Tan, Liam Hayes and Luke Robbins.

12-13th October 2019
AllAid First Aid (https://www.allaid.com.au/) at North Turramurra
Participants: Aidan Cameron, Alexandra Repetto, Ava Del Tufo, Beth Howlett, Brendon Yiu, Evie Wilkins, Glenn Southern, Greta Ritchard, Jeffrey Kwan, Jenny Stansby, Joshua Yang, Liam Viney, Matthew Notarangelo, Nathan Jensen, Nick Fabian, Nicolas Di Campli, Oliver Nicholls, Scott Koppelhuber, Stephen Roche, Yvette Mascarenhas.

December 2021
Participants: Ashleigh Ford, Beth Howlett, Brendan Conneely, Jenny Stansby, Juri Hemmi, Maria Lastra Cagigas, Mira Jordan, Nadav Cohen, Nat Shroeder, Oliver Nicholls, Stephen Roche
6-9th February 2023
Wilderness First Aid Australia (https://www.wildernessmedicine.com.au/) at Mount Victoria
Participants: Amelia Kaag, Angela Ha, Brendan Conneely, Gabriel Dickinson, Georgie Clare, Jayden Maisel, Katie Wilson, Linna He, Mali Woods, Nadav Cohen, Samantha Millard, Zenon Platritis
26-28th May 2023
Wilderness First Aid Australia (https://www.wildernessmedicine.com.au/) at Mount Victoria
Participants: Amelia Vasiliou, Bennett Frerck, Caitlin Donovan, Felix Kibblewhite, Daniel Gilbert, Krishna Srivastava, Lloyd Siharath, Maddi Dunster, Margot Mason, Ryan Van Dyk

17th June 2023
A First Aid Simulation Day was run by Katie and Oliver to share, retain and regain First Aid and Situational Management skills with club members and trip leaders. Check out the blog post below!
15-17th December 2023
Wilderness First Aid Australia (https://www.wildernessmedicine.com.au/) at Mount Victoria
Details: Remote Area First Aid | 15th -17th December 2023 – UNSW Outdoors Club
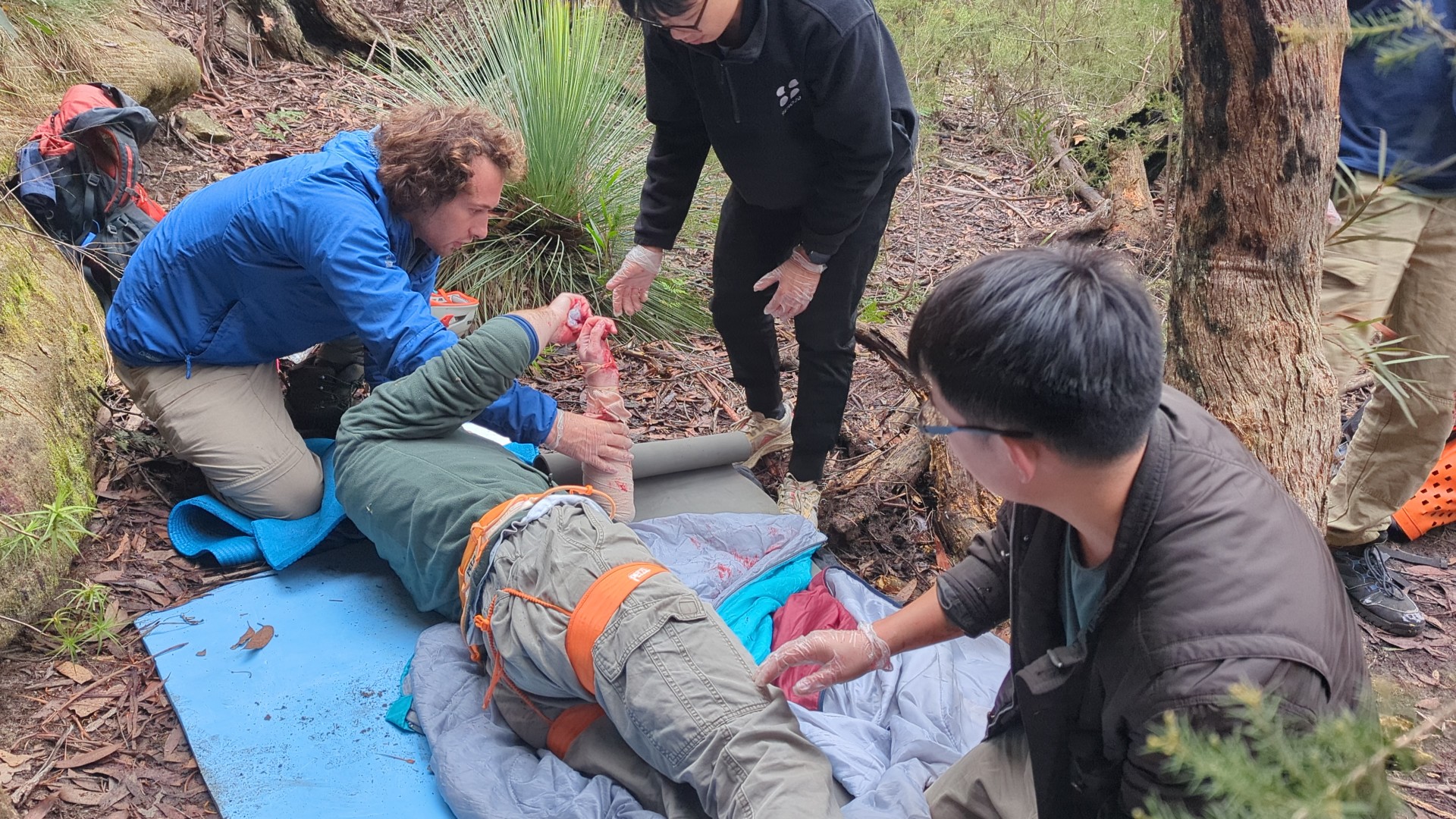
16-18th May 2025
Wilderness First Aid Australia (https://www.wildernessmedicine.com.au/) at Mount Victoria
A three-day RAFA course which included among others: basic life support, triage, and assessments; physical trauma and managing bleeds, burns, and shock; managing hypothermia, stroke, anaphylaxis, and other medical issues; CPR.
Participants: Sudarshan, Grant Z, Leo J, Michael A, Marley SM, Stephanie S, Evan H, Zee, Adam R, Jack P, Micah W, Jack M, Ella P